Epiphysiodese
Today’s case of the week is about a 14-year-old patient. The young man had suffered a so-called patellar luxation (dislocated kneecap) with immediate reduction while playing soccer. Within 2 weeks, I suffered another patellar dislocation, this time while running. The patient was fitted with an orthosis outside the clinic and presented at our surgery for further clarification.
Investigation
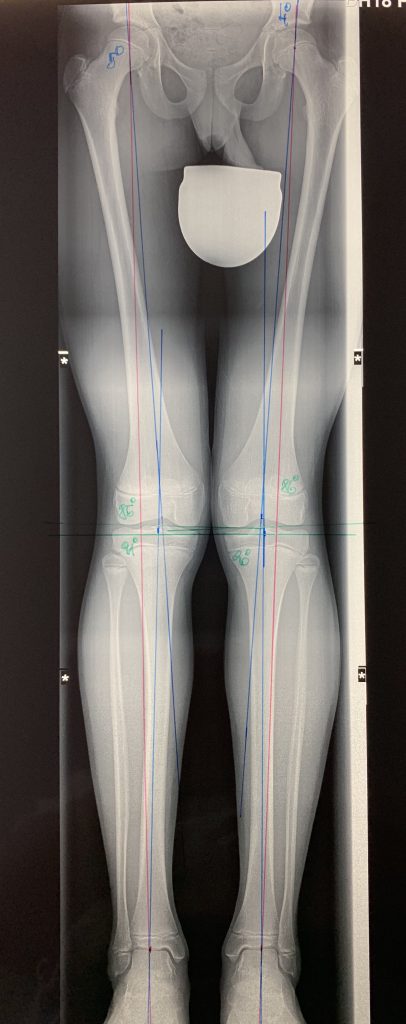
The clinical examination already showed a valgus leg axis, so-called knock-knees and a significantly increased mobility of the kneecap. A whole-leg X-ray allowed the leg axis to be measured precisely and 5° valgus was detected on both sides. A magnetic resonance tomography of both knee joints showed the bruise marks of the patellar dislocations that had occurred in the form of bone marrow edema and additionally a flat trochlea femoris (sliding groove of the kneecap on the thigh).
Diagnosis
The patient’s X-B position causes an outward pull on the kneecap when the thigh muscles are tensed and, in combination with the flat sliding channel, causes the kneecap to pop out.
Treatment
Due to the young age of the patient and the existing residual growth potential, a temporal epiphysiodesis has been carried out. The growth plate on the inside of the knee was temporarily blocked with special epiphysiodesis plates without damaging the growth plates. This results in further length growth on the outside of the knee and the existing knock-knee increasingly becomes a straight or slight bow leg.
Postoperatively, regular whole-leg X-rays are taken to monitor changes in the leg axis and, if the bowlegs are sufficiently corrected, the epiphysiodesis plates are removed again.