Habitual patellar luxation – Trochlead dysplasia
Our Case of the Week is about a patient who suffered a traffic accident in 1995, ruptured his posterior cruciate ligament, and reported problems in his right knee joint during sports practice ever since. Compared to the anterior cruciate ligament, the posterior cruciate ligament is much more strongly developed and therefore much less frequently affected in injuries (ratio 1:10). It is also interesting to note that the sex ratio of ACL injuries is 1:4 females vs. males.
As a mechanism of injury, a so-called dash-board-injury often occurs. This means that in the course of a high-rasance trauma, the lower leg is displaced backwards in relation to the upper leg. As with our patient, this often happens in traffic accidents.
Treatment approach
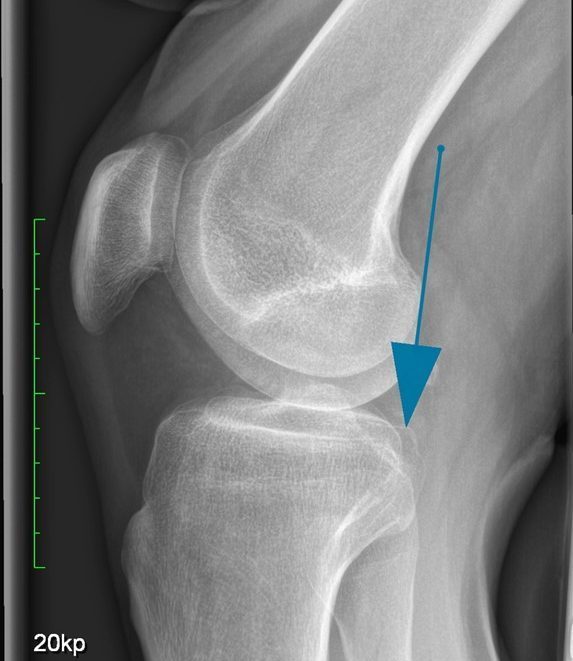
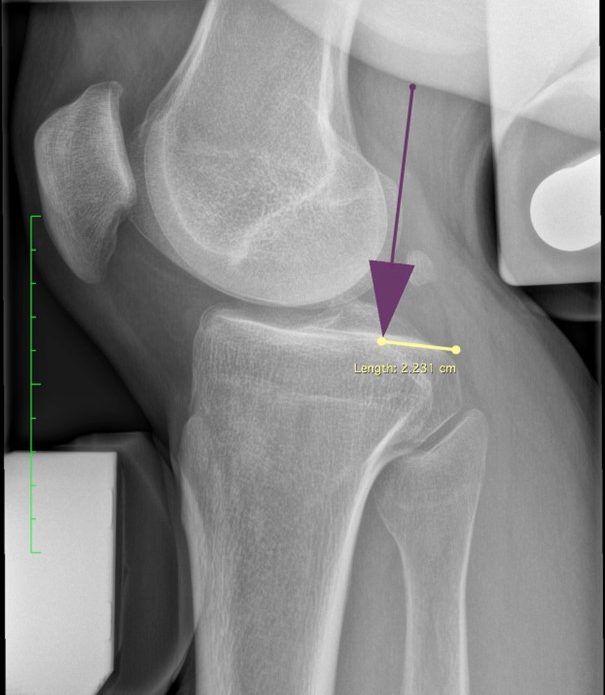
The diagnosis is made by a precise clinical examination in which the posterior drawer is assessed in lateral comparison and in different rotational positions of the lower leg, MR tomography, as well as by held radiographs in which the displacement of the lower leg in relation to the thigh (which is limited by an intact BUA) is measured. Physiologically, the displacement distance is a maximum of 3mm. On our patient, the rear drawer is 22mm. If the posterior drawer is greater than 15mm, surgical rehabilitation is mandatory to achieve improved function and sports fitness.
Treatment approach
Often, a posterior cruciate ligament rupture can be treated conservatively by means of orthotic fitting for 3 months. If chronic instability remains, surgical reconstruction is necessary. Because our patient presents with existing discomfort during exercise due to instability in the left knee joint, posterior cruciate ligament reconstruction was recommended.
In surgical reconstruction, the posterior cruciate ligament is replaced with a tendon from the patient’s own body, similar to the treatment of an anterior cruciate ligament rupture. Unlike the anterior cruciate ligament, however, the graft used must be longer, so the combination of semitendinosus and gracilis tendon is suitable.
Intensive physiotherapy follows postoperatively to enable a gradual return to athletic exertion as soon as possible. The duration until complete healing and regaining full sports capability is usually 9 to 12 months.